
Parish AIDS projects make an impact

 SACBC AIDS OFFICE EVALUATION
SACBC AIDS OFFICE EVALUATION
SMALL GRANTS PROJECT
SUPPORTED BY CATHOLIC RELIEF SERVICES
Time frame being evaluated: 2009 to 2013
OCTOBER 2013
“We stand with, we want to be with the little ones, the people who do not count, who will never be listened to because they are not given access to anything or any structure; those who are lost in some outlying rural community or urban slum which will rarely, if ever, be visited by anyone;
the little ones who end up simply being a number, a statistic whether it be in terms of the escalating infection rate or in terms of the escalating numbers of dead in the mortuaries awaiting a pauper’s funeral, sometimes for months on end because families cannot be traced.
We want to be with the poorest and alienated communities, to be present to and involved with them in their reality.”
Bishop Kevin Dowling, Rustenburg
 Facilitated and documented by Rosanne Shields
Facilitated and documented by Rosanne Shields
shieldsr@mweb.co.za; 021 462 4555
Rural Development Support Programme
1. INTRODUCTION & BACKGROUND TO THE EVALUATION
Rural Development Support Program (RDSP) was commissioned by the SACBC AIDS Office to facilitate an evaluation of the AIDS Office’s small grants programme, which is supported by Catholic Relief Services, for the period 2009 to 2013. In the AIDS Office’s proposal to CRS the following strategic objectives are listed:
– Diocesan and small projects are able to provide HIV care and support to areas in greatest need through accessing funding from the SACBC AIDS Office.
– Lobbying and advocacy at national, provincial and local level to increase resource mobilization is strengthened.
– Diocesan and small projects have increased capacity to implement good quality programmes.
Therefore the two focus areas for this evaluation were the grant making and capacity building roles of the AIDS Office, within the context of the small grants programme.
The main aims of the evaluation were:
– To develop a profile of the small AIDS projects working at diocesan/local level, looking at their broad achievements, challenges and prospects for future survival.
– To outline what role a national AIDS office should be playing and to measure the achievements and difficulties of the SACBC AIDS Office against this.
– Once the bigger picture of the AIDS sector at a national and local level within the Church has been analysed, to measure the activities of the small projects programme against the CRS Proframe of 2009-2013.
– To raise any issues relating to the internal functioning of the AIDS Office at a participatory staff session.
– To note any recommendations for the AIDS Office’s work at the local level in future.
The evaluation included the following methodology and activities:
1. A participatory staff session to assess the achievements and challenges of the AIDS Office and to establish what information from the local level would be most useful. This took place on the 7th of August at Khanya House and included Sr Alison Munro, Johan Viljoen, Nondumiso Jwara and Geraldine Hedley.
2. Site visits in the Eastern Cape to Care Ministry (Port Elizabeth) and Ntaba Maria Clinic (Queenstown).
3. Site visits in KwaZulu-Natal to Noyi Bazi Clinic (Pomeroy), Ithembalethu Outreach Project (Estcourt), Asiphile eSt James (Lamontville, Durban) and St Nirvards (near Umzinto).
4. Questionnaires were sent to the following 13 projects, seven of which responded (in bold):
– Nazareth House AIDS Project, Cape Town
– Diocesan Welfare, Polokwane
– Mercy Clinic, Pretoria
– Kopano Lerato, Pretoria
– Nzhelele (Kurisanani) HBC, Tzaneen
– Vezokuhle HBC, Witbank
– Diocese of Keimoes-Upington
– Diocese of Franscistown
– Rorising Man & Youth, Klerksdorp
– Christ the King Parish, Manzini
– Caritas Swaziland HBC
– Regina Mundi Garden Project, Manzini
– Thandukupila AIDS Project, Mariannhill
5. Questionnaires were also sent to the following resource people:
– Bishop Jose Luis Ponce de Leon
– Sr Hermenegild Makoro
– Joan Marston, HPCA
– Peter Modiselle
– Fr Joe Kizito
– Fr Gregory Mkhize
– Sr Anita O’Leary
– Zibu Mgadi
– Sr Christine Jacobs
Within this group the rate of response was disappointing, probably due to other work pressure or perhaps because some did not feel qualified to comment on the work of the office. However responses from Sr Hermenegild, Peter Modiselle and Sr Anita O’Leary were very helpful. Bishop Jose was not available to comment.
6. Reading of all documents shared by the AIDS Office to track progress, identify changes in the context and way of working since 2009 and develop background information.
7. A request to CRS to receive their feedback and for them to raise any concerns.
As part of preparing for the evaluation, Sr Alison Munro made the following important points:
– Due to the global financial crisis and a decrease in the funding made available to CRS by its private donors, the amount of the grant awarded for this programme was cut annually, limiting the number of projects that could be supported and the amounts paid to each one. This was a situation beyond the control of CRS and the AIDS Office.
– The pool of projects supported by the office varies, from those who have very little other support to those who have performed and developed well enough to be scaled up to receive larger support, for example from Global Fund or PEPFAR, also through the AIDS Office.
– Constraints experienced by the AIDS Office included a limited budget, poor capacity at local level with insufficient oversight in some places, high training and monitoring costs and its own staff related difficulties in the early years of the grant.
– Despite these constraints, a variety of diocesan and parish-based organisations in South Africa, Swaziland and Botswana have provided home-based care, orphan care and treatment services. They have also been assisted with retreats, capacity building, home-based care supplies, awareness-raising of HIV/AIDS and TB, and infrastructure improvements.
– The AIDS Office must now define its niche for the future, as the HIV/AIDS landscape has changed, with far less AIDS funding available and the state having launched the roll-out of ARVs.
Feedback from Loreshnee Yirefu of CRS was as follows:
The AIDS Office’s reporting is on track, with Nondumiso Jwara doing a very good job. She has organised a lot of training and site visits and knows the projects well. Nondumiso took part in a project management course with CRS and was the second highest scorer.
Geraldine Hedley’s financial reports are excellent. CRS has seen great improvements in the reporting and accountability system of the AIDS Office since the mid-term review. The capacity building that has taken place at small project level has been highly valued and very empowering. From CRS’s point of view this has been a great project.
Acronyms Used
OVC
HBC
ARV
ART
VCT
TB
CRS
DSD
SASSA
CATHCA
RDSP
Orphaned & Vulnerable Children
Home-Based Care/Carer
Anti-Retroviral
Anti-Retroviral Treatment
Voluntary Counselling & Testing
Tuberculosis
Catholic Relief Services
Department of Social Development
South African Social Security Agency
Catholic Health Care Association
Catholic Health Care Association
Rural Development Support Program
2. SUSTAINABILITY DISCUSSION
On 7 August the facilitator met with Sr Alison Munro, Johan Viljoen, Nondumiso Jwara and Geraldine Hedley, as the SACBC AIDS Office staff most involved with the Small Grants Project, to discuss the evaluation and to look specifically at the internal functioning of the office. As pointed out at the mid-term evaluation, there are many factors that determine whether an organisation will be sustainable. RDSP has grouped them according to the following categories and these were used to gain feedback from the AIDS Office staff:

The following areas emerged as noteworthy:
Management Board
This structure works well and is fully functional, with two liaison bishops, the SACBC Secretary General and Associate Secretary General. Having this body in place helps with communication and accountability. The office has its own non-profit organisation number, which also helps with specific fundraising activities.
Staff Training
The training provided by CRS has been very useful and different staff members have attended.
Succession Planning
This is always a difficult discussion when an organisation is so well established and some staff members have been in place for a long time. It was felt that it is human nature for leadership skills to be vested in one persona. However in the case of the AIDS Office it was also felt that enough had been invested in others for things not to fall apart should a key staff member leave. Delegation of tasks is sufficient and the four staff involved act at a middle management level. The depth of skill and leadership within the office has improved over time and there is better combined knowledge. The staff meeting every Monday contributes greatly to this and everybody is aware of what the next person is doing. The staff prefer a less “line manager” and more collective approach. That being said, many Church agencies are currently run by strong personalities and their absence would be keenly felt.
Staff
Retrenchments have taken place due to a lack of funding, so the office is not as large as in previous years. It was agreed that performance appraisals could happen more often and some debate took place about the best approach.
Programmes
The office has developed a more balanced and strict approach to working with projects at community or diocesan level. The staff have felt the need to be more challenging in making sure projects meet their responsibilities, for example in the use of a grant or training received.
Capacity Building of Target Group
The challenge is to get people to use the training and general capacity building they have received. It was agreed that it is important to set assignments during and after training and to screen those who are coming to the training to make sure they are the right people. It was also pointed out that mentoring visits have been very important and absolutely key in building capacity. A significant improvement in reporting and monitoring and evaluation at site level has been noticed by the office staff. Most sites that have received mentoring have improved their output.
The fact that some projects have been “upscaled” by the AIDS Office to receive bigger funding contracts from the likes of the Global Fund and PEPFAR is a major indicator of improved capacity. This is where the small projects grants have been so useful, in preparing projects for greater, more complex support.
Research
There is a lot of research available in the HIV/AIDS sector, so the AIDS Office has chosen to focus on what is most needed and useful. The office has been part of appropriate publications and helpful information is accessible on their website.
Funding
The current thinking within the AIDS sector is that, with South Africa’s ARV programme in place, the role of home-based carers should change from caring for people with AIDS-related illnesses to screening for diseases such as TB, carrying out voluntary counselling and testing for HIV and assisting people with ARV adherence. This thinking is in line with the Department of Health. With the roll out of ARVs in South Africa, international donors are on the whole seeing the HIV/AIDS pandemic as under control and are providing less assistance. Therefore it is very important for those working in the sector to re-define their mission and find their niche. For the AIDS Office this is likely to be focusing on working with the most vulnerable children.
Projects working at community level also need help in redefining themselves now that the funding landscape has changed and people generally have access to ARVs, although in some areas this is still patchy. It was pointed out that the fact that many people choose not to know their status or go onto ARV therapy because of the stigma still attached to HIV would not be enough to persuade donors to fund the fallout of AIDS, such as the need for home-based care. In other words, the message coming from outside is that people will simply have to overcome the stigma if they want to survive.
Clearly there will be a lag period between acceptance of this theory and reality on the ground. This is where training of former home-based carers to act as community health workers is so important, as one of their key roles is to help people with diagnosis and adherence to treatment. (There is feedback on this from project level in this report.)
What the AIDS Office would like to see is movement in Church projects, in line with a changing AIDS landscape. For example, moving from giving out food parcels to vulnerable households to including them in child development programmes. An important role will also be to assist and encourage projects to access corporate support for their development work.
Budgets
The staff interviewed felt there has been an excellent adaptation by the office to the funding situation, which has required adjusting to the new demands of funders and the support available. A flexible strategy has been needed and fortunately the office has some reserves to fall back on.
The budget for the small grants project is clear for the staff, including how each small grant is to be used. This is closely monitored.
Target Group
There is a good level of trust within the target group and the site visits have really helped with this. This was reflected by the projects visited as well.
Networks
AIDS is one sector where you cannot work alone. Involvement from many parties is required and working with government is essential. Relationships with the various departments vary from province to province and even at district level. It is very important that projects themselves be part of networks at the local level, for example with the Dept. of Health. National level networks do not replace what can be achieved at ground level. The AIDS Office has always been active on AIDS structures.
Profiling
The office has made great strides in the use of social media, with a lot of interaction taking place on facebook. The website is kept up to date and used to access articles and research information. The website is administered by Mariannhill Mission Press and feedback from them, according to google analysis, has been excellent.
Planning, Monitoring & Evaluation
There is a strong culture of this, as both a management tool and donor requirement. Staff seemed comfortable with following this cycle. Projects receiving a small grant also report monthly and this helps with building their capacity to communicate with other funders too.
Policies & Procedures
These need to be updated according to recommendations from PEPFAR. This is required for the whole of Khanya House and is being worked on.
3. INFORMATION FROM SITE VISITS: PROFILING PROJECTS WORKING AT LOCAL LEVEL
RDSP visited the following six projects, all of which have received various forms of support from the SACBC AIDS Office. The visits were very valuable in understanding the context in which many of the projects work and seeing first-hand the kinds of activities they are carrying out. These six can be viewed as a sample of the support work of the AIDS Office. The six site visits were particularly enlightening as they provided a very real picture of the type of project typically supported through the small grants programme, either through a grant or capacity building. The challenges faced by these projects are complex and their sustainability, particularly from a financial point of view, is tenuous.
Ithembalethu Outreach Project, Estcourt, KwaZulu-Natal
The project is run by Sr Maureen Aron, who has just the right personality for this kind of work. She has an amazing ability to view the whole person, with great respect and care, and her approach is an example of what can be achieved with very few resources. She spoke of mixing small vials of aqueous cream for patients with sore feet or rashes and how touching them and talking and praying with them is so important for their spirit. This is where the Church’s extra level of care for mind, body and spirit shines through. Sr Maureen also sees it as her task to train her staff so that the project does not fall apart if she is not there.
At Ithembalethu there are 12 carers working with 100 patients (trained by Sinosizo, Durban, now defunct). Patients are visited according to categories: Category 1 (once/month), 2 (twice/month), 3 (once/week, only 2 at present) – with category 3 being the worst. Fortunately, because a good relationship has been built up, they work closely with the local hospital and clinic sisters on TB testing. 398 people are currently on ARVs through the local clinic and Ithembalethu monitors and supports them. The ARV clinic sometimes has some logistics problems, such as the flow of medicines. Sr Maureen has seen the impact of the ARVs, with far fewer deaths, down from 10 per week when she worked at hospice to one a month now. There is a major impact of poverty and alcohol use on people’s wellbeing, interacting with the ARVs. ARVs are sometimes stolen by children to smoke, so adherence for the whole month is difficult. There is also not enough general help at the clinic, for example if people have flu or an opportunistic illness.
The project is trying very hard to introduce the concept of “one home, one garden”, getting people to grow cabbage, spinach and beetroot (the project also has its own small garden). Water has to be manually collected in two informal settlements, making gardening challenging.
Sr Maureen believes the move from home-based carers to community health workers will take time. The project is preparing carers with a range of skills and new information – each month they have input. Hygiene issues within the home also need attention (linked with personal dignity). She emphasises to the carers that treating the whole person is vitally important. She is very worried about the breakdown of family life and the deterioration of moral norms and values. She told us about stopping her car at the side of the road as a mother was beating her son. She asked her why she was doing this and she said he had been caught having sex with another boy. They were both younger than ten. Ithembalethu now aims to work with the community on issues of dignity and the protection of children. They will be workshopping issues of self-respect and sexual education with children directly.
There are 191 OVC in the programme, up to the age of 15 years. ID documents have been secured and the children have a sense of belonging. Two Christmas parties for 40-50 children took place, provided by the board and parish. The children also benefitted from the winter hampers (tracksuit, shoes, scarf, underwear, gloves, socks) distributed by the AIDS Office, which also sponsored a sports day.
Sr Maureen stated that the AIDS Office is a great help, providing moral support, alleviating the feeling of working in isolation. Johan Viljoen’s visit was highly appreciated. Management training provided by the office has been very helpful. Financial systems have been developed and she is training the other staff now. The retreat day was very necessary and helpful (carers pray with the patients and read the bible). The AIDS Office also sponsored World AIDS Day activities which were very successful, with lots of talks and patients sharing stories. She would like more Durban meetings organised by CADACC (Catholic Archdiocese of Durban AIDS Care Commission), but realises funds are low. It is good for diocesan projects to get together for mutual support and sharing of programmes.
One of Sr Maureen’s biggest strengths is her networking with local businesses and Catholic resources (she could give lessons on this to other projects). She draws her board members from the parish and has somebody helping her with fund raising. Examples of support from local businesses include 200 5kg bags of mielie meal donated from SASCO per month, toys from Checkers for OVC and party packs from the local pharmacy. After visiting a patient at home who was living in absolute squalor, with her children, Sr Maureen decided to rope in the local hardware store and the school to build a new structure as part of Mandela Day.
Ithembalethu have applied to the Dept. of Social Development for a grant to subsidise the programme and it is possible this will be approved. The Dept. of Health provides some help with materials for carers. The national lottery requires two years of audited financial statements, so when these are ready they will apply for a vehicle. There has been particular support from Durban North parish with blankets and food.
Sr Maureen’s strengths include supervision/oversight, record keeping, holding carers accountable but caring for them (she removes labels off white blouses donated in order to create uniforms). She would love to supply them with proper uniforms and refreshments in their small staff room in order to encourage them.
Noyi Bazi HBC Clinic, Pomeroy, KwaZulu-Natal
This clinic is in a particularly remote area on the way to Tugela Ferry. We met with Sr Madelaine who explained that the first clinic had opened in this area in 1964. Later government opened clinics and provided maternity services. At the present day clinic the staff sometimes see 200 patients per day. There are 3 peer educators and 3 people doing VCT. The clinic has 4 professional nurses on a government grant. Patients pay a small fee. The future of the clinic is uncertain as government is building a 24 hr care centre on a site opposite Noyi Bazi, to be finished next year.
Noyi Bazi has 40-50 home-based carers, with 10 on the TB screening programme and 20 receiving stipends from the Dept. of Health, via the SACBC. The original HBC training was done by CATHCA. There are 1000 patients on ARVs at this clinic, with the drugs supplied by government. Operation Hunger provides a soup kitchen three times per week. Sr Madelaine’s observation is that those who take ARVs and have food are doing alright, but if they don’t have access to decent nutrition there is a problem. There is also a tendency to go back to traditional healers and the two don’t mix, interfering with adherence. There is also the problem of denial, with people not wanting to know their status. Sr Madelaine also pointed out that it is a pity the main focus is always HIV when there are many other chronic illnesses, like diabetes and high blood pressure, especially amongst the elderly. It is important not to forget about them.
The clinic and its associated programmes are always working with uncertainty regarding funding and how long resources will last. Many of the carers are themselves very poor and they cannot afford to give them much. A carer sometimes ends up poorer than an OVC. Noyi Bazi has in the past managed to build 5 houses for HBCs from a private donation. The relationship with the carers can be tricky as it is 100% voluntary. The dignity of being recognised is very important. Within the broader community there is a problem of apathy and the need to motivate people, which is difficult. Finding leaders is difficult as people are frightened of taking this on. There are many concerns around the abuse of the social grants system, where a vicious cycle is created by people having children to get a grant. The clinic is serving a wide area, where unemployment is likely to be as high as 80%. There is a reliance on social grants, e.g. a pension supports the entire family. Sometimes people stop taking their medication so as to qualify for the HIV grant, which is renewed every year. So the health of the person at the annual review is important. The staff also carefully monitor the distribution of food parcels, re-assessing who needs them most.
The clinic has an outreach programme for OVC. Those running HBC and OVC meet weekly.
A monthly visit to an identified area takes place where the children gather for activities, HIV & TB education and a meal cooked by the home-based carers. Peer educators attend as well. Saturdays are spent with children, volunteers run activities, work in the garden and help with homework. 10-12 young women volunteers meet every month for in-service training. There are even 2 soccer teams and another group does cultural dancing with the OVC – this came out of the Saturday sessions. At Christmas all OVC come together in the hall (over 500). Homeplan housing is underway, starting with 5 but aiming for 50. Twenty houses were built previously through the SACBC. There is good co-operation with the local school regarding OVCs and the programme helps those in grade 12 with career advice.
Noyi Bazi has regular contact with the AIDS Office, especially Johan. This is a good relationship, helpful and understanding. They attend capacity building training and find it helpful. The home-based carers report back on workshops at monthly meetings. They struggle at first to implement what they have learnt and need follow-up. The Winter Warmer hampers from the AIDS Office helped the OVC programme.
There is a fairly good relationship with the Dept. of Health, working with the district health office. Inspections and training take place. Sr Madelaine believes the clinic’s statistics are good for them. However she finds it difficult to get social work assistance from the Dept. of Social Development and this is frustrating. They try to resolve problems themselves and the HBCs take children to Tugela Ferry for ID docs etc. Businesses help out at Christmas time – Nando’s in Dundee sponsored 120kgs of chicken. A local clothing supplier helps out where she can and the Peace Corps come from Tugela Ferry to teach sewing skills, hoping to develop some self-reliance.
Asiphile eSt James, Lamontville, Durban, KwaZulu-Natal
The project started operating in 2008. There are 10 volunteer HBCs who were on CATHCA–provided stipends until these ran out. They are visiting 40 patients each regularly, most with HIV and/or TB, some with strokes. There is a HIV+ support group, doing handiwork to generate income. The products, such as bags, looked good. The project has an excellent relationship with the local clinic and they work together on awareness raising. The clinic sisters come and do VCT and TB screening. They work on a mutual referral system.
Asiphile eSt James is the only provider of home-based care in Lamontville, which is densely populated. The carers were trained by Sinosizo, an organisation that they miss.
People are accessing ARVs at the local clinic, with two former caregivers from this project working there. The project promotes adherence and distributes the nutritious meal replacement, Sejo. This is badly needed. ARVs are generally working very well and the death rate has dropped a lot. There is VCT at the clinic, but at awareness sessions the mobile clinic does this. The co-ordinator, Sr Bhengu, said there is far less stigma attached to HIV in a city situation. She and the chairperson we met with also spoke about the unemployment in the area and the fact that a lot of people are dependent on grants, using the child support grant for the whole family.
The project includes 200 OVC, with a soup kitchen for them after school twice per week. There is also a holiday programme, psychosocial support and AIDS awareness. There is a lot of assistance provided to OVC to obtain their official documents. Operation Sukuma Sakhe under the premier’s office is working very well – departments co-operate to clear administrative bottlenecks. Asiphile eSt James is working very well with the library next door and sometimes the parish supports the co-ordinator with petrol money. The project works according to events in the health calendar.
There is a very good, appreciative relationship with the AIDS Office. The AIDS Office has supported a sports tournament during the world cup, winter clothing for OVC, infection control kits (Dept. of Health as well) and Sejo porridge. The retreat for carers was very useful, but could have been longer. Because of cash flow it is not always possible to pay transport upfront for AIDS Office workshops and then be refunded.
R60 000 was received from Mondi, and it is hoped that this will be renewed. SAPREF (refinery) is building a new centre on the next door site which will make a big difference to the space available. A computer was provided by CADACC. Sr Bhengu would also like more networking and sharing with others, but there is a shortage of funds for this.
St Nirvards, near Umzinto, KwaZulu-Natal
St Nirvards is also based in a remote area, about 40 minutes from Umzinto by car, in the middle of a sugar cane and forestry area. The project has 9 home-based carers, with stipends from the Dept. of Social Development, plus 15 volunteers. The carers also work with senior citizens and there is HIV/AIDS awareness raising, based on Education for Life, carried out at weekends. Support groups for people with HIV have been formed. TB patients are referred to the local clinic if symptoms are visible during visits. Although the project is very short of funds, which we could see, a large area is covered on foot. The clinic helps people referred by the community care givers, but it would be helpful for the community care givers to give their patients referral letters and identify their work to the clinic. They are not well known at the clinic. The staff have been working for four months unpaid. Only DSD funds come in and they are waiting for the latest re-imbursement.
ARVs are available at the nearest clinic but the number of people choosing to go onto treatment is not growing. There is still a stigma attached to testing. The project is working on this problem, and sees support groups as very important for this. They are trying to motivate people to go to the clinic for testing. The Dept. of Agriculture is helping a little with a small garden at the centre but water is a problem. St Nirvards is encouraging people to grow their own gardens.
The project is working with 300 OVCs – this was 560, 260 have been referred to government services. They have a very good relationship with DSD, SASSA and the Dept. of Home Affairs, the premier’s office and the local municipality. A soup kitchen is run for OVCs with food from DSD. St Nirvards tries to help school-going children through volunteers and to advise them when they finish school. They badly need support for awareness events, as well as school uniforms. Children drop out of school if they don’t have uniforms. There is a big difference in the lives of OVCs receiving healthy meals and access to grants. Access to SASSA grants is generally good. Bursaries are needed for studying beyond grade 12. The co-ordinator, Bheki Mthembu, is planning a child protection campaign but needs funds (in his experience an event is not successful unless refreshments are provided).
The AIDS Office training in counselling and testing and proposal writing was well received. There is also good support from the bishop’s office. However Bheki feels there is not enough support from the Mariannhill co-ordinating office and prefers to work with Nondumiso at the AIDS Office.
Jumpstart Foundation supported the costs of erecting the building the project occupies and they received an Umzumbe grant in aid to buy the fridge and computer. They badly need to negotiate for electricity. It is an Eskom supply area but the electricity has not been connected. They are asking the municipality for their help with this. The Dept. of Health supports events by addressing people and they supplied First Aid kits.
Further training needs include how to handle children who are vulnerable, how to get them to open up and talk about their challenges. Also how to pick up and handle the abuse of OVC grants at home.
Care Ministry, Port Elizabeth, Eastern Cape
Working in a more urban setting, 93 volunteer caregivers are providing care and support within specific communities, including emotional support, health education, home-based care and ARV adherence support. Twelve were on a stipend from the Dept. of Health (national). A category system works well:
Category A: purely voluntary (11)
Category B: Paid R300 per month, work 16 hrs per month with 4 different clients (42)
Category C: Paid R750 per month, work 48 hrs per month with 8 different clients and do 20 screening questionnaires per month (30)
DFID TB programme: Paid R1000 per month to do TB screening, must cover 6 people per day and work every morning (10).
The volunteers are clustered into 11 areas and supported by a registered nurse. They receive on-going training. Care Ministry is trying to improve the health of the volunteers too, including fitness and, starting this year, self-defence. According to Siobhan Dooley, the fundamental role of Care Ministry is to support the work of the local clinics. The health screening tool used encourages re-testing, empowers clients to know and understand their CD4 counts and viral loads and identifies defaulters. There has definitely been a reduction in the number of patients with extended illnesses at home in need of home-based care.
There has been a shift in focus to preventative screening. Treatment education and adherence has become the biggest need and much more of a focus.
There is a huge problem of defaulters in the community and a lack of understanding of CD4 or viral loads. The clinics are refusing to release these test results to patients, it is not clear why. This is a big problem as it prevents people from really understanding their particular virus. There is a desperate need for nutritional support but funders have withdrawn support for this. There is also a growing problem of TB in households.
The roll-out of ARVs is good, but red tape can be a problem. People are generally not taking personal responsibility for their own health. The reasons for this include a lack of education, apathy, not being able to or wanting to take time off work to go to the clinic, side-effects of medication (although these have lessened). The one-pill treatment is not widely available yet. There is a “learnt helplessness” in some communities. Some people also go off their ARVs for a period in order to lower their CD4 count before the annual social grant assessment.
There is a major concern that as resistance to ARVs becomes a problem we are going to start seeing more people sick at home again. Some initial medical trials have highlighted a number of children resistant to AIDS medications.
OVC receive emotional support, home-based care, school support, adherence support and there are guardian support groups in place. About 200 children have been referred to schools. Families are taking in more and more children then battling for resources. Some guardians are very receptive to learning about how to care for the children, however there are still children living with guardians who don’t care enough. It is a battle to get information from the clinics regarding a child’s health.
Support from the SACBC AIDS Office led to the launch of the DFID TB Project. The learnings from this project impacted on the development of the new health screening tool.
220 to 240 people are screened per month, with 25-30% testing positive for TB when they reach the clinics. This initiative has been very successful at helping people to take charge of their TB situation. The AIDS Office also funded spiritual retreats enabling stress relief for volunteer caregivers, as well as the World AIDS Day programme. The office also assisted with World TB Day, held in partnership with Red Cross, which included TB screening at the taxi rank in Uitenhage. The AIDS Office introduced Care Ministry to Capacitar and Moira Boshoff is now a trainer in this methodology. They also assisted with office equipment.
Rapid HIV testing training was offered for the TB volunteers (and was very useful) but Care Ministry had serious concerns about how the TB volunteers would carry out the 50 hours practice required without antagonising the Dept. of Health, which has not given the go-ahead for this. A delicate balance of co-operation has to be maintained and the department prefers that rapid testing happens at their clinics.
The Care Ministry networks very well in Port Elizabeth. Home Based Care Forums are going in Motherwell and Walmer and often have a spiritual element. Strategic networking with major organisations takes place. They network with Red Cross and St Francis Hospice as they are dealing with TB at different stages. Care Ministry is also a training provider for grassroots projects including King William’s Town Diocesan AIDS Project and Hospice, Somerset East. There is an excellent relationship with the Dept. of Health and Care Ministry is well known to them and supported. The relationship with the local municipality is not very helpful and they are bankrupt anyway.
Other funders include Misereor, who have supported their work with OVC for 7 years and general funding from the lottery. Score (UK) has provided about 2000 pounds, Missio funds home-based care and the Dutch Catholic Church has donated EUR 2400.
Ntaba Maria Clinic, Queenstown, Eastern Cape
Ntaba Maria is a home-based care project that started in 2004, funded by the AIDS Office. Care givers carry out home visits, monitoring patients, sorting out medication, TB screening and distribution of food parcels. Through the use of Sejo and ePap the project aims to boost the nutrition of HIV and AIDS patients. The Heaven Outreach Programme based at Kuzigudu village is supported by the Diocese of Queenstown. At Ntaba Maria there are two nursing sisters, five trained caregivers and one volunteer.
The roll out of ARVs has changed the HIV/AIDS situation, but not that much, as people still need to be educated about the importance of taking their ARVs. At least some people do take their ARVs regularly and even encourage those who are still in denial to come forward. The challenge is that when people get better they go back to big cities (e.g. Cape Town) and stop taking their medication. When they come back they are in a very bad state health wise, usually even on their death beds.
There are many orphans left behind by those who have died of AIDS. Caregivers assess their conditions and network with social development for social grants and birth certificates. They are also helped with school uniforms and social gatherings, such as Christmas parties. The number of OVC is still growing because some of them are coming from the city to the villages so that the grandmother can look after them. The only change is that those who are infected are keen to take their medication – the challenge is to tell them what the medication is for as they do ask questions.
Since the project started in 2004 the AIDS Office’s support has helped tremendously, impacting greatly on people’s lives as they feel they can disclose their status and they take their medication regularly. People generally prefer to use the Ntaba Maria clinic rather than government clinics as they feel that confidentiality is taken seriously. HIV and AIDS training has been received from the department of health. They also attended training courses with RDSP on financial management, fundraising, proposal writing and report writing. The project can now do its own bookkeeping and the books look good. Governance is still a challenge.
There is a good relationship with other AIDS projects in the diocese and DSD and the Dept. of Health refer people to them. Some Catholic families help with food parcels, Dept. of Health funding has been received through CATHCA and some funds have come from Kindermissionwerk.
4. INFORMATION FROM QUESTIONNAIRES
In addition to the site visits, questionnaires were sent to thirteen projects, with seven being returned. These seven were:
Nazareth House, Cape Town
A registered children’s home and place of safety, catering for OVCs who have been statutorily placed into their care in terms of the Children’s Act (Act 38/2005). Many of these children are HIV infected and are on ARVs. Several are also physically and/or mentally disabled, needing special care 24 hours per day. Nazareth House also counsels and encourages the family members of these children where possible, although in most cases they have been unable to trace family members. The staff visit schools, youth groups, etc. when invited, to give information and education on HIV/AIDS.
Diocese AIDS Ministry, Diocese of Keimoes-Upington
A home-based care project including ten home-based carers delivering services in different communities in the Kai! Garib Municipality area – this is their main focus. Counselling
(VCT) is run at different clinics, with three trained counsellors at Lutzburg, Kenhardt and Augrabies. A counselling service is also provided at the ART outreach point in Keimoes and on-going counselling is done at the office. Every second Monday the ministry runs treatment outreach at Keimoes Clinic. ART clients receive transport from their homes to the treatment site and back. The home-based cares/counsellors also assist the treatment team by helping them with the observation of HIV/AIDS clients. All special days are observed at the treatment site, such as World TB day in March and World AIDS day in December. The ministry serves soup and sandwiches as clients leave home early and might not have something to eat. On Thursdays they transport HIV/AIDS positive clients from home to the clinic. On these days clients receive adherence counselling and preparation for ART Treatment
The OVC Programme strives to help children by securing IDs, birth certificates and social grants. Eleven caregivers provide psychosocial support. The caregivers on this program are also part of meetings and sessions held by the office. The AIDS Ministry manages three soup kitchens in and around Keimoes, providing a meal to clients four days per week, as well as information and awareness sessions. When possible clothing and blankets are distributed.
Mercy Clinic, Winterveldt
Mercy AIDS Services are attached to Mercy Clinic and there is a strong referral system among the Primary Health Care, the TB Clinic, the Ante Natal Section and the HIV/AIDS Department. The Home-Based Care Program offers clinical, physical, spiritual, psychological and social care services to the community. There are HIV/AIDS prevention and education workshops for youth and other groups. There is an ART Clinic, with support groups.
Kopano Lerato OVC Programme, Winterveldt
Working with OVC through educational support, HIV prevention education, home visits, child protection workshops, general health care (health talks, TB screening and accompanying children to the clinic), psychosocial support and general counselling. There are four OVC support groups, divided into age groups and a special one for children and their guardians on ARVs. A drama teacher runs arts and culture sessions, the children play sport and do traditional dancing.
Nzhelele Home Based Care (Kurisanani), Tzaneen
Kurisanani in the Diocese of Tzaneen exists to provide a holistic, effective and compassionate response to the HIV and AIDS pandemic, including through home-based care programmes, ART treatment rollout and OVC programmes, including monitoring of OVC, educational support, shelter, psychological support, home economic strengthening and health care support.
Vezokuhle Home Based Care, Witbank
This programme carries out very important awareness raising campaigns, including teaching orphaned and vulnerable children. They encourage the HIV positive support group to adhere to their treatment.
Diocesan Welfare, Polokwane
Provides holistic home, parish and community care to people with HIV/AIDS and their families. They identify people within the community with leadership qualities in order to train them to co-ordinate groups in their own community, with the purpose of supporting those with HIV/AIDS. They also provide training in peer education. They take care of the elderly, disabled and OVC.
The following is a summary of the feedback received:
Examples of the impact of the support received from the SACBC AIDS Office:
• Generally the financial support provided by the office has helped to pay stipends, cover programme costs, train staff and cover admin costs.
• In some cases a specific programme, such as home-based care or OVC, has been earmarked for support.
• General support of caregivers has also been important, whether through debriefing, training or retreats.
• One project said “our work became easy” because of help with practical needs such as centre renovation, household items and kits.
• The particular impact of support on children was highlighted, through their care and shelter.
• Site visits were also highly valued – this is where the office has built up trust and opened communication.
• Support has also been provided with auditing, supervising and advising HIV/AIDS work. “Support of any form has enabled us to make a difference to and in our patients’ lives…giving them development and empowerment opportunities.” – Mercy Clinic
• A specialist area of support has been in the handover of ARV sites to fall under government jurisdiction. From Kurisanani: “The support given by the SACBC when developing our relationship with the Department of Health was excellent. As a result, MOUs were signed and treatment, bloods etc. were accessed…words cannot express the support given”.
Reflections on training programmes the projects have benefitted from:
• Financial and administration skills training was mentioned by most respondents and this was found to be helpful.
• Specific training in home-based care, TB management, VCT and rapid testing was also highly valued and essential to the proper functioning of caregivers.
• Retreats for carers were very successful, giving them a sense of being valued for work that is not always remunerated.
• The Kopano Lerato OVC programme gave a comprehensive listing, which reflects the variety of training carried out, funded or organised by the AIDS Office: project management, child & youth care, HIV counselling & testing, peer education, memory work, monitoring & evaluation skills, food gardening, psychosocial support, human/child trafficking, financial management, career guidance, staff retreats.
• Others mentioned management & governance, basic computer skills, resource mobilisation and palliative care.
• Clearly days such as World AIDS Day and World TB Day have been harnessed to run events and create awareness. The office has assisted with these.
• Those running an ART site have had specific training in related skills.
• “Through the training made available to our staff they have been helped to improve themselves and uplifted our standard and quality of work.” – Mercy Clinic
• At project level skills are also being passed on to others by the more established organisations, such as Nazareth House: “We partner with a caring organisation in offering training for carers here at Nazareth House. Also, our trained carers working in the field of childcare are participating in an on-going specialist childcare training programme from our senior childcare worker and social worker. This includes all aspects of caring for children with HIV and AIDS.”
Role of a Diocesan AIDS programme:
• In an urban setting, pulling together a network of HIV/AIDS projects is a more straight forward task. Nazareth House reported that in the Archdiocese of Cape Town they are in the process of establishing a Health Desk which incorporates the previous CAN (Catholic AIDS Network). It was felt that AIDS should no longer be dealt with separately from other health issues, as all have an impact on each other and are very often interlinked. These gatherings are also times for spiritual renewal and growth.
• The role of a diocesan AIDS programme like Kurisanani is to source funding and distribute resources to the parishes through which they work and then to monitor and evaluate this. All projects which receive funding report to Kurisanani, who in turn report to the SACBC AIDS Office.
• Unfortunately we did not receive responses from the Diocesan AIDS Office in Aliwal North or CADACC.
Changes in the needs of home-based care since the roll out of ARV treatment:
• Nazareth House expresses the change very clearly: “Home based care has changed dramatically in our area, due to the improved health of those infected with HIV. Whereas previously most home-based care was very much “hands-on” physical basic nursing care, the emphasis is now more on emotional support, encouragement and supervision of daily medication & diet etc.”
• Diocesan Welfare, Polokwane, see themselves as educating clients and supporting the treatment centre.
• Kopano Lerato: “Since the roll-out of ARVs the death rate in both children and parents has gone down and the opportunistic illnesses decreased. The children who are under the care of foster parents are no longer a challenge or as big a burden on the extended families. One of the reasons being that they now are able to access ARVs and there are not so many severe and debilitating illnesses around. Also, mothers are living longer and are able to care for their children, leaving fewer orphaned children.”
• Vezokuhle HBC say the situation has changed a lot and Kurisanani say that the home-based carers are seeing people living and getting back on their feet. Their role then is more focussed on adherence to treatment.
• Mercy Clinic: “Since the roll-out of ARVs patients’ lives have improved, we have more mobile patients and our bedridden patient numbers have decreased. Patients’ families have taken responsibility for their ill loved ones, there is more hope all round, both those infected and affected feel less vulnerable with a more positive outlook. The extended families and guardians are less burdened…” They also reported that the HIV/AIDS rate in their area has decreased from 1 in 3 being positive to 1 in 4 testing positive. Couple’s counselling has also improved.
• In Keimoes a major part of their role is to support and complement the Dept. Of Health with the ARV programme through counselling and adherence support.
The situation for children orphaned or made vulnerable by AIDS (OVC) and what has changed over the last few years:
• In Polokwane resources are needed to care for children adequately.
• For Kurisanani the situation continues to be one of great need. While more organisations have come on board in response to the needs of OVC, they are only managing to meet the needs of a relatively small group.
• Kopano Lerato are encouraged by the fact that orphans are more integrated into the community and there is less discrimination against them. They had reported being discriminated against because of their social status, physical appearance and living conditions. “Over the last few years this has changed because of ARVs and the help the SACBC has given us to help build and refurbish homes for the children and their extended families.”
• In Keimoes through the support of the Dept. of Social Development they can run an effective OVC programme.
• At Nazareth House they have seen a marked decrease in the number of infants and children being admitted into their care with stage 3 & 4 AIDS. Their death rate for HIV infected children has dropped by 90% (the only deaths over the past few years being due to parental neglect and defaulting of a child’s treatment prior to admission). Another positive change is the increased level of awareness and support for infected mothers and their children which is developing within the local communities and welfare organisations in and around Cape Town. The stigma is also becoming less of an issue, and fewer mothers are abandoning their HIV infected children. In addition, the mothers themselves are remaining healthier and stronger because of their own ARV treatment.
The number of non-infected orphans (due to parental AIDS-related death) has also decreased, to a lesser degree.
Working relationships with the Dept. of Health, the Dept. of Social Development & local municipalities:
• This ranges from a simple referral system and working together on awareness campaigns, such as for Vezokuhle HBC, to a more intensive relationship such as for Nazareth House, which is the only after-hours place of safety in the city area for abandoned babies and OVC. They work closely with the local SAPS and Child Protection Services but, apart from a minimal monthly subsidy, they do not receive any additional funding.
• The Diocese AIDS Ministry in Keimoes works closely with both the Depts. of Health and Social Development, as does Mercy Clinic. They all provide different support systems and a strong referral system is in place.
• Kopano Lerato relate well to the Dept. of Health and use the clinic when the children are sick. The clinic also assists with support group talks, with counselling and by checking health conditions. The Dept. of Social Development helps with the applications for social grants and with referrals. One of the local social workers is a board member. The department has also helped with money for stipends for the carers. Networking with the local municipality takes place through the Community Child Care Forum. A mobile Home Affairs facility comes to the area and helps with the registration of births and applying for ID books.
• Kurisanani’s relationship with the Dept. of Health is particularly good but the Dept. of Social Development is “nowhere near being able to support any programmes concerning OVC”.
• For Diocesan Welfare, Polokwane, the relationships are quite simply “bad”.
Other support for work at project level:
All of the projects are feeling the pinch financially and are constantly under pressure to raise sufficient funds for their work. Some of this comes in through concerted fund raising efforts or events. Other sources of funding include:
• National Lottery Distributive Trust Fund
• Catholic Relief Services
• Local businesses
• Religious congregations
• A specific OVC donor
• Private donors
• Local clinics (with donations in kind, such as gloves)
• Dept. Social Development (soup kitchens & OVC)
• Independent Development Trust
Two of the seven projects responding to the questionnaire said they had no other support other than that of the AIDS Office.
5. FEEDBACK FROM SR HERMENEGILD MAKORO, SACBC SECRETARY-GENERAL
“There is respect and great regard for human dignity. As a Church we are indeed thankful to God that we were able to save so many souls.” Sr Hermenegild
The feedback of the SACBC Secretary-General is very important in measuring the work of the AIDS Office as the office falls very much under her leadership. This was a conscious decision by the bishops – that their response to the AIDS pandemic should be through their own office rather than a more independent associate body. Sr Hermenegild says: “The Church has made a big mark in caring and addressing the scourge. The efficiency in which the sites have been run is remarkable. Not only efficiency in doing the work but the care, respect, delivering of medication on time and availability of the staff is a big contributing factor.”
She values the care of OVC, not only their access to food, but the skills and other support they have received. She sees the AIDS Office staff as having a very good relationship with OVC. OVC have received much attention needed from the sites: feeding schemes, afternoon supervised studies, career camps have made a big change in their lives. Material needs have been provided e.g. birth certificates, school uniforms, warm clothing in winter. Lately there is a housing project for orphans in order to give them a decent home. For Sr Hermenegild capacity building has been one of the main areas that the office focused on. “It is amazing that so much caring work has been covered by using people who don’t have much education.”
However the secretary-general is also very concerned about the future: “I am not sure at the moment as to how the office will continue as funding has been drastically cut down. With little funding available in the future I would like to see moral and spiritual support being given to the care givers. If the office would instil in people’s minds that taking care of the orphans or HIV/AIDS patients is a ministry and not that money comes first. At present the good work has been done because there have been incentives but in the future there might be no money but we will still be faced with the same problems.” She is concerned about the dependency of the sites. The office cannot go on supporting them indefinitely. She also asks the question whether the building of houses for OVC should fall under the AIDS Office or be tackled by one of the other agencies.
6. CAPACITY BUILDING CARRIED OUT BY THE AIDS OFFICE
“Whatever we have been invited to and that has been made available to us from the AIDS Office we have joined in, related well to it and have been greatly helped.” Mercy Clinic
As Peter Modiselle, one of the people who has carried out training for the AIDS Office points out, its work is necessary and important, particularly with the size of the Catholic Church. It is able to reach a large number of people both HIV positive and negative. From his training experience, the AIDS office should offer on-site technical assistance to all the areas they operate in. Emphasis should be placed on smaller/rural areas of the dioceses where there are HIV/AIDS and OVC programmes. He recommends that the AIDS Office maintain capacity building, as well as governance initiatives, undertaken in the previous years, including on-site audits. These provide a source of reference as to the status and size of each of the projects/dioceses funded. All trainers would agree that capacity building is not a once-off type of training or on-site technical assistance but on-going support that must be done continuously.
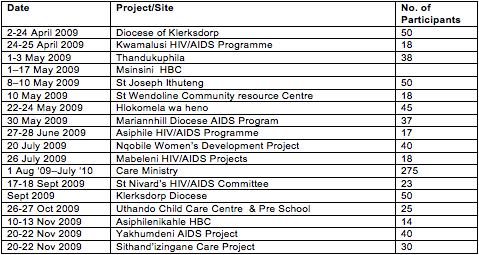
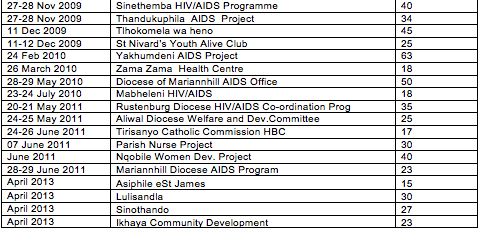
The following capacity building activities were carried out or organised by the SACBC AIDS Office during the evaluation period of 2009 to 2013:
WORKSHOPS AND TRAINING
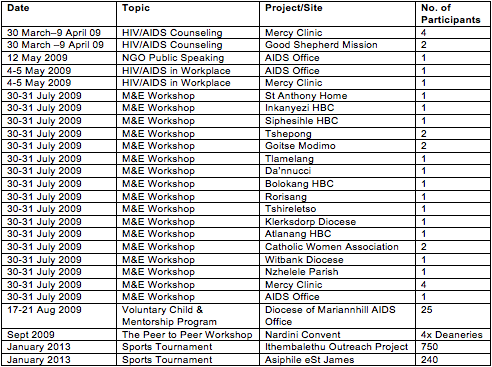
2013 WORLD TB DAY (MARCH)
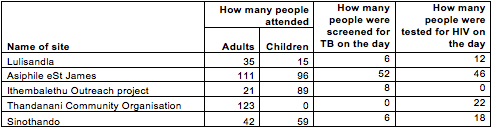
2013 TRAINING

RETREATS FOR CAREGIVERS & PROJECTS
7. ALLOCATION OF SMALL GRANTS BY THE AIDS OFFICE
As stated in the AIDS Office application to CRS, it is the small projects providing small scale day to day services to those in need that can make the difference in people’s lives. According to UNAIDS, over the last three decades small community-based projects have been the key providers of prevention services, treatment, care and support. In countries like South Africa, Botswana and Swaziland, their impact is magnified by the reliance on them by some of the most hard-to-reach individuals.
The UNAIDS Best Practice Collection has featured the SACBC AIDS Office and pointed out that “One of the major advantages of the Church as an institution responding to the HIV epidemic within the Southern African context is an extensive, well-established network among congregations throughout Southern Africa, including some of the most isolated and under-developed communities in the region.”
Using this network, between 2009 and 2013, the AIDS Office distributed R9 069 284.00 in small grants to eligible projects. These are all listed in the attached appendix.
Bishop Kevin Dowling sums up the work of the AIDS Office, including the impact of distributing small grants: “We stand with, we want to be with the little ones, the people who do not count, who will never be listened to because they are not given access to anything or any structure; those who are lost in some outlying rural community or urban slum which will rarely, if ever, be visited by anyone; the little ones who end up simply being a number, a statistic whether it be in terms of the escalating infection rate or in terms of the escalating numbers of dead in the mortuaries awaiting a pauper’s funeral, sometimes for months on end because families cannot be traced. We want to be with the poorest and alienated communities, to be present to and involved with them in their reality.”
8. OUTCOMES OF THE EVALUATION
• Reports written by the AIDS Office show a model of the office as an incubator of small projects that can grow to more independence. Subsidiarity has been a key theme running through the office’s work. This is essential as, with the demands of working in the AIDS sector, dependency on a national office is something that happens very easily. Inevitably some projects will survive beyond the lifespan of their existing resources, be these grants from the AIDS Office or government stipends, and others will shut down. The training provided by the office has aimed to alleviate this as much as possible by focusing on governance, raising resources and acquiring better technical skills such as monitoring adherence to ARV treatment and screening for TB.
• The fact that a significant number of projects have been “up-scaled” to received more complex and larger grants from PEPFAR and Global Fund is a key indicator that growth within the projects has taken place and that the small grants approach of CRS has leveraged other support.
• In this regard it is important to remember that some of the projects can train others and to draw on them at a regional level. A good example is Care Ministry in Port Elizabeth. Perhaps it is time to investigate who could do what in the way of training their peers and to make a database of this so that not all of the training required falls to the AIDS Office to supply or organise.
• Many of the projects are going to need help with bridging the gap between the work they have been doing in the way of HBC and what they now need to move into, such as helping people with adherence to ARVs and preventative screening. There is still enough of a resistance to testing and treatment within the community, as well as some patchy ARV supply areas, to put a lot of pressure on the projects to keep supplying HBC services as before. The AIDS Office knows this and is factoring it in to their capacity building, as can be seen from the focus of the training in 2013. However perhaps the pace in closing the gap will be slower than expected.
• Related to this is the fact that the projects expressed how important moral support is, especially from national level and from the diocese in which they operate. Even if this support does not come with a grant, it is still needed and helps those on the frontline to feel part of a larger struggle as Church. Other SACBC agencies can and do help with this support and some very productive relationships have been built up over time.
• In “Continuing the Mission of Jesus”, Sr Alison points out that at the August 2004 SACBC plenary session the bishops resolved to strengthen the work on AIDS within the dioceses by ensuring that committees and co-ordinators are in place at the diocesan level. It is not clear how much this has been achieved or how successful the co-ordinators have been but it seems that fulfilling this resolution has been full of challenges, probably most of them relating to the funding required to sustain this middle layer. While it would be ideal to have such committees and co-ordinators, it is the individual projects that have endured and it seems that this is where future investment should be. Perhaps strong projects can be tasked with reaching out to weaker ones in the same diocese.
• One of the main focus points of the office has been funding and organising retreats. These have been highly valued and have helped to prevent burn out amongst the many caregivers on which the Church’s response to HIV/AIDS has relied.
• The on-site visits and mentoring carried out by AIDS Office staff has been highly valued by the projects and has led to their strengthening. The relationship between them and the AIDS Office (which they often simply call the SACBC) is excellent, with a high level of trust. This makes it all the more important that, as the availability of small grants diminishes, the projects be assisted in other ways and kept within the fold.
• It has been documented that many projects working with children affected by AIDS originated in home-based care programmes. The AIDS Office has seen an increase in the number of projects responding to the needs of orphans and vulnerable children. This is particularly important within the context of South Africa where children in general are extremely vulnerable. Rates of child neglect and abuse have reached grotesque levels – this week alone saw the discovery of two toddlers, raped and murdered, and then dumped in a public toilet cubicle in Diepsloot. Our children and young adults are badly in need of help, particularly those who carry the added burden of AIDS within their families. It seems this is a key and obvious area in which the AIDS Office should continue and amplify its involvement.
According to this evaluation, the strategic objectives of the 2009-2013 SACBC AIDS Office-CRS Proframe have been achieved and the constraints encountered have been well dealt with. The CRS-AIDS Office partnership has changed lives and achieved an enormous amount in the fight against HIV/AIDS through the support of projects at ground level.